Research
BREAST
Background
Breast cancer is a malignant tumour that originates in the cells of the breast. It is one of the most commonly diagnosed types of cancer among women. The lifetime risk of developing breast cancer in industrialized countries is at a level of one in seven women. Early detection and diagnosis are of key importance for effective treatment of breast cancer. However, current diagnostic methods are insufficient to detect all breast cancers in time. This is mainly shown by the condition that we fail to prevent metastatic spread and to adequately monitor treatment. Consequently, new methods are required to improve early cancer detection in a screening setting and after detection to guide and monitor treatment. Ultrasound imaging might be an excellent choice since it has low costs, is real-time en does not use hazardous radiation. However, ultrasound imaging lacks adequate specificity and requires well-educated radiologist to interpret breast ultrasound images. Therefore, our research goal is to improve the detection, diagnosis and monitoring of breast cancer using ultrasound imaging and related methods. Furthermore, we aim to develop low-cost ultrasound and CAD systems to facilitate breast cancer detection for health care workers in developing countries.
Methods
Ultrafast ultrasound imaging
The automated breast volume scanner (ABVS) is capable of recording ultrasound images of the entire breast that can be evaluated afterwards by radiologist to detect suspicious lesions. One of the limitations of this scanner is the long scan times up to 90 seconds to record one volume. Those long scan times introduce breathing artefacts and, consequently, possible lesions can be missed and misclassified. We are developing ultrafast ultrasound imaging techniques (LINK: quantitative) to decrease scan times to a few seconds without compromising and even increasing the image quality (contrast and resolutions).
Quantitative ultrasound
Quantitative ultrasound is another option to improve the specificity of ultrasound images. In 3D ultrasound, accurate discrimination of small solid masses is difficult, resulting in a high frequency of biopsies for benign lesions.
Therefore we explored and incorporated the Computer Aided UltraSound (CAUS) protocol (developed for hepatic steatosis classification) to enable quantitative and relative expression of the echolevels using a reference phantom method. We adapted the software such that ik could handle 3D ultrasound (US) volumes originating from the Siemens ABVS system, and made it a generic method by expressing echolevels relative to a reference phantom. From the 3DUS images the relative echolevel statistics as well as the "residual attenuation coefficient" were estimated after manual deliniation of the suspected lesions in 3D. Furthermore we incorporated echo level features like the peritumoural surrounding (PER) and posterior-tumoural phenomena (POS) echo level.
Hybrid tomosynthesis-ultrasound system
After a suspicious lesion is detected by tomosynthesis, it is often further evaluated using ultrasound imaging to determine whether it concerns a breast cancer or a benign lesion. Consequently, women have to be recalled after a tomosynthesis image is made for an ultrasound exam. To simplify this procedure, we aim to develop a hybrid tomosynthesis-ultrasound system in which tomosynthesis and ultrasound images are obtained almost simultaneously. The advantage is that the radiologist can simultaneously evaluate images of both devices. In this way, an unnecessary recall can be prevented and the procedure time reduced. Furthermore, some lesions are hardly visible on tomosynthesis but can be seen on ultrasound or vice versa. In our research, we are developing ultrasound scan acquisitions to reduce the scan time and to increase the image quality especially at lower depths (up to 10 cm). We are also investigating the addition of ultrasound elastography and Doppler imaging to further improve the performance of this hybrid system.
Breast Volumetric Imaging for Biopsy Navigation
After imaging with mammography, ultrasound (US) imaging of a lesion with subsequent breast biopsy is common clinical practice to determine whether the lesion is malignant or benign. Among available breast biopsy techniques, ultrasound-guided core needle biopsy (CNB) is preferable. However, this technique cannot be applied if the lesion is US occult (not detectable in the echogram), and the radiologist has to perform MRI-guided biopsy that is time-consuming and cost-ineffective. The objective of the MRI-Ultrasound Robotic Assisted Biopsy (MURAB) project is to facilitate US-guided biopsy even for US occult lesions and simplify the work of radiologists. The procedure comprises 5 major steps: MRI imaging, ultrasound volumetric imaging, MRI-US image fusion & lesion localization, needle navigation, and biopsy. The MURAB project involves 5 partners (Radboudumc, University of Twente, University of Verona, Siemens Healthineers, KUKA robotics, and Medical University of Vienna), who work in collaboration on the MURAB clinical setup. In the MUSIC group, we focus on the development and validation of methods for breast automated volumetric imaging for US -MRI image fusion. We are working on complimentary approaches: breast 3D-US imaging with an automated cone-base scanner and breast 3D-US imaging with free-hand volumetric ultrasound.
Results
Ultrasound image quality
In our studies, we compared the image quality between ultrafast ultrasound (plane-wave) imaging and the currently used conventional focused acquisitions in the ABVS system. Our results suggest that ultrafast imaging will enable breath-hold ABVS examinations, eliminating breathing artifacts while otherwise preserving similar image quality (contrast and resolution). Therefore, 11 steering angles were used in ultrafast imaging resulting in an 18 times increased frame rate. We showed that the frame rate and ABVS transducer moving speed did not significantly affect the image quality (Figure 1). Currently, we are investigating several reconstruction and filtering methods to improve the image quality in ultrafast ultrasound imaging Quantitative Ultrasound.
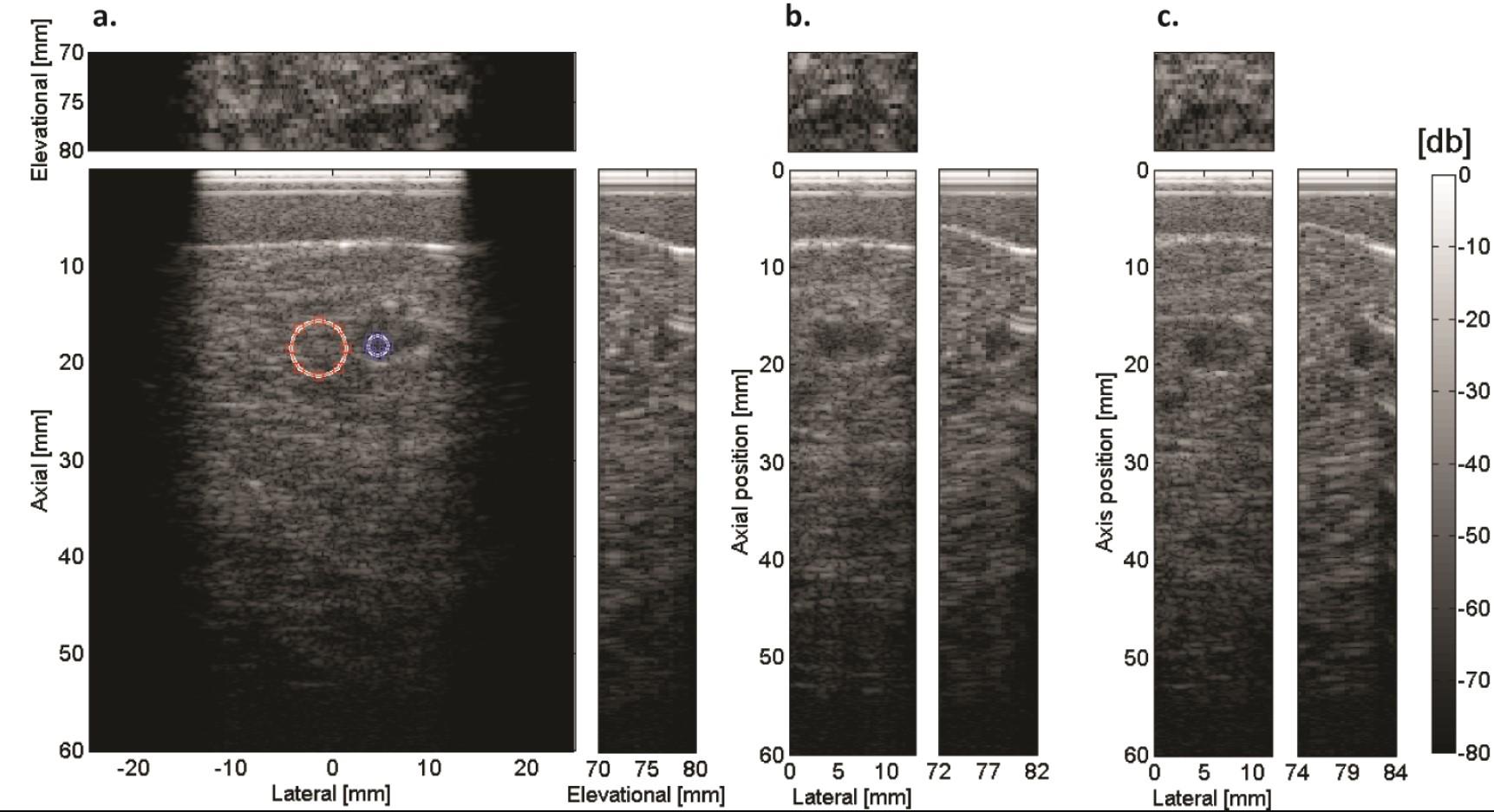
Coronal (up), transverse (down left) and sagittal (down right) views of a cyst extracted from a 3-D breast phantom volume acquired by moving the transducer by: a) 10 mm/s, b) 20 mm/s and c) 50 mm/s. In the first image CNR measurement positions are indicated (blue: cyst, red: background). In b) and c), only the area around the cyst is shown (Hollander et al., 2016).
Quantitative ultrasound
We applied 3D quantitative breast ultrasound (3DQBUS) to 3D US studies of 112 biopsied solid breast lesions with a size smaller then 1 cm. The resulting features were used for classification of the lesion by a logistic regression analysis. The classification accuracy was evaluated by leave-one-out cross-validation. The area under the ROC curve was 0.86 for both readers. 3DQBUS is a promising technique to classify suspicious breast lesions as benign, potentially preventing unnecessary biopsies (Meel et al. 2017).
Breast Volumetric Imaging for Biopsy Navigation
We developed different scanning approaches. Results show volumetric images of a custom-developed phantom, scanned with an ultrasound transducer mounted on a robotic arm (top) and with a transducer integrated in the wall of an automatically rotating cone-shaped container (bottom). More results of the cone-based volumetric ultrasound breast imaging scanner have been published in (Nikolaev, 2021)
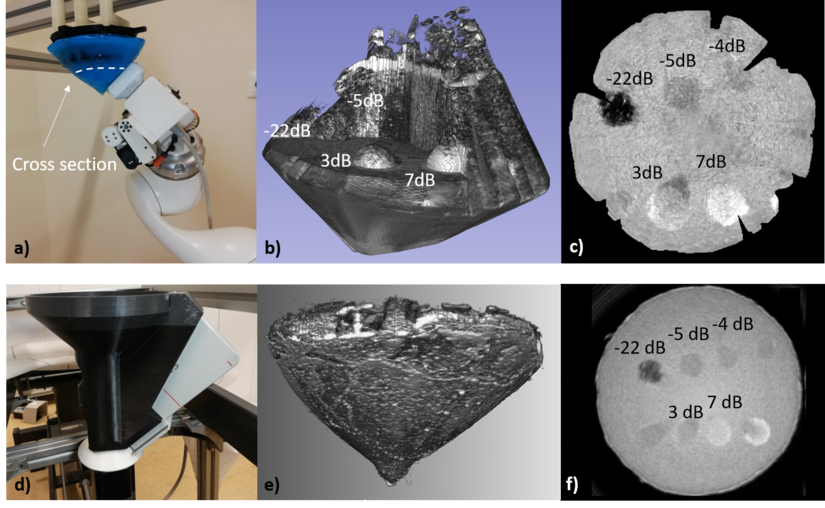
Volumetric imaging of the breast volumetric phantom with the robotic arm (top) and automated cone-shaped container (bottom). From left to right: the imaging setup(a, d), rendered volumetric data (b, e), and coronal cross-sectional image (c, f).
Subsequently, we co-registered in-vivo MRI and 3D US data in a volunteer with a benign lesion (fibroadenoma) and a cyst. The same cross-sections were taken for clear observation of the fibroadenoma and the cyst. Dark areas in US images represent fat, while bright areas represent glandular tissue. Both fibroadenoma and cyst are visible as dark spots and pointed out with arrows. In the MRI images (T2 sequence Dixon protocol, fat), glandular tissue is represented as a shaded area while bright represents fat. Both lesions are visible and characterized by dark spots. The skin layer is occult in the utilized MRI image.
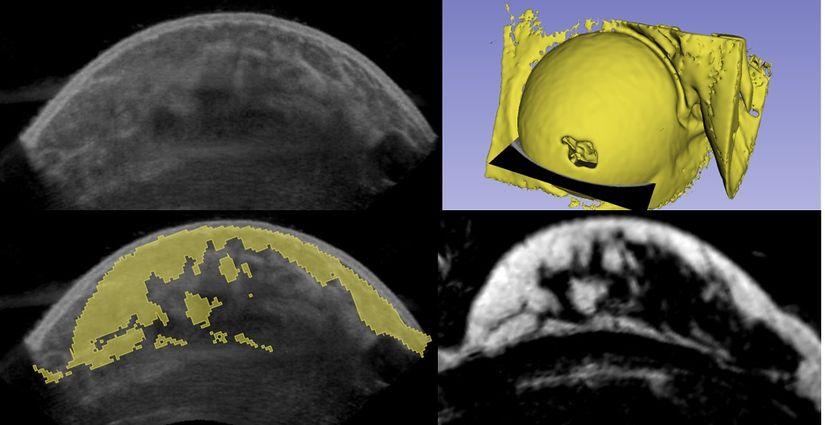
MRI-3D US image fusion of a breast. a) Rendered MRI data with indicated cross-sectional transversal plain. b) Cross-sectional US image. b) Cross-sectional MRI image. c) MRI data overlayed 3D US data.
Funding
- X-US: Combined ABVS and Tomosynthesis scanning (supported by Siemens Healthineers, active)
- 3D FUSION BREAST: 3D Functional UltraSound Imaging Of Nodules in BREAST (supported by Dutch Technology Foundation and Siemens, finished)
- MURAB: MRI and Ultrasound Robotic Assisted Biopsy (supported by Horizon 2020 (688188), Siemens, and KUKA, active). MURABproject.eu