Research
CARDIO-VASC
Vascular strain
Cerebrovascular accidents (i.e. strokes) with an annual incidence of 13.7 million people are the second leading cause of death and disability worldwide. A large part of cerebrovascular events are caused by the rupture of carotid artery plaques. To prevent (recurrent) ischemic strokes a carotid endarterectomy (CEA) is performed. Clinical risk stratification in these patients is mainly based on the stenosis degree (geometry, maximum blood velocity) caused by the atherosclerotic plaque and clinical risk factors, such as hypertension and hyperlipidemia. However, this risk stratification is rather suboptimal since there is more and more evidence that, regardless of stenosis degree, plaques containing a lipid-rich core covered by a thin fibrous cap (vulnerable plaques) are more prone to rupture than plaques mainly containing fibrous tissue (stable plaques). Therefore, other parameters are needed to identify vulnerable plaques and, with that, improve (individual) clinical care.
What has been done
In vascular ultrasound, research interest has shifted from stenosis degree to plaque composition, geometry, and deformation. Since lipids are softer than fibrous tissue, it can be expected that vulnerable plaques deform more than fibrous plaques in response to the pulsating blood. Over the past years we developed different two-dimensional techniques, called compound ultrasound strain imaging and shear wave elastography, to characterize tissues non-invasively. With these methods, it is possible to determine parameters related to the elastic properties of carotid plaques in order to identify the vulnerable ones. To bring these techniques to 3D, the frame-rate needs to be boosted by using ultrafast ultrasound techniques.
Our research aim
Our current research aims are:
- to further develop and validate the 2D techniques (i.e. strain and shear wave elastography) in patients with atherosclerotic diseases and show the relation between measured values and cardiovascular events in order to establish new prognostic markers.
- to extend the already developed 2D technique to a 3D technique to be able to localize the most vulnerable part of a plaque, if present, in 3D.
Methods
In- and ex-vivo clinical studies are being performed in order to validate the in-patient performance of the developed 2D technique in patients and to link the strain or shear wave measures to the cardiovascular risk profile of patients. However, to bring this technique to 3D, high frame rates are required. To achieve this, plane wave transmission (one transmission over an entire region instead of multiple focused ultrasound pulses) with displacement compounding is used to measure with a high frame rate and sufficient image quality, in 2D. To extend this method to 3D, either 1) a linear array probe is translated along the elevation direction, or 2) a 2D matrix probe (fully populated or row-column array (RCA)) is used with which multiple plane waves are transmitted and the echo data is coherently compounded in receive to improve the contrast and lateral/elevational resolution.
Results
A first in vivo validation study of compound strain imaging showed that the technique allowed successful differentiation between plaques with a large lipid pool and fibrous plaques with a sensitivity, specificity, positive and negative predictive value of 85%, 71%, 81% and 77%, respectively (Hansen, 2016) . The first in vivo application of 3D strain measurements with as linear array showed distensibility values matched with previously published values, while the corresponding volumetric principal strain maps revealed locally elevated compressive and tensile strains (Fekkes, 2019). The first simulation study with a RCA showed displacement/strain values closely following the ground truth.

Figure: Histology (right), conventional b-mode incl Doppler (middle), and elastogram (right) of a fibrous carotid plaque (upper row) and atheromatous plaque (lower row),
revealing high strain values in the lipid core and low strain values in fibrous plaque components.
Funding
- Characterization of atherosclerotic plaques in the carotid artery using non-invasive ultrasound elastography (VIDI grant of the Netherlands Organisation for Scientific Research NWO and the Dutch Technology Foundation STW and Philips Medical Systems, finished)
- Ultrafast imaging, the next level of cardiovascular diagnosis (VICI grant of the Netherlands Organisation for Scientific Research NWO and the Dutch Technology Foundation STW, finished)
- Ultra-COMPASS: Ultrafast ultrasonic compound push wave imaging and strain estimation for personalized stroke risk stratification (Radboud Institute of Health Sciences Junior researcher project 2019, Radboudumc, active)
Cardiac Strain
Cardiovascular disease is one of the leading causes of death in the Western World. In the Netherlands 20.000 people die each year of an acute myocardial infarction or stroke. Two-dimensional ultrasound has been the most widely available imaging modality to evaluate cardiovascular structure and function. Improvements in two-dimensional ultrasound image resolution have led to more detailed imaging of the myocardium, heart valves, vessel walls, and atherosclerotic plaques. Doppler techniques are readily available to estimate the blood flow and pressure gradients across heart valves and vascular stenoses. However, two-dimensional B-mode images have a limited reproducibility in three-dimensional structures and do not (yet) allow for detailed tissue characterization.
Specifically, in cardiac function analysis, the standard volumetric biplane measurement of ‘ejection fraction’ to determine systolic function has an inter-rater and longitudinal variability of 5-10%, due to apical foreshortening, suboptimal endocardial contouring and changes in pre- and afterload. Furthermore, it is a rather late marker of systolic dysfunction, knowing that the complex orientation of cardiac muscle fibers allows for compensation of ejection fraction when certain fibers become dysfunctional.
What has been done
In cardiac ultrasound, two-dimensional myocardial deformation (strain) imaging, by means of tissue doppler imaging and now speckle tracking, has found its way into the clinic. Global longitudinal strain (i.e. shortening of the total muscle length in longitudinal direction) has been shown to aid in the prediction of cardiac events and mortality in various cardiac diseases (heart failure, valve disease, postoperative), especially when ejection fraction is still preserved. Furthermore, it is possible to assess regional wall motion abnormalities (lower strain, pre-stretch, post-systolic strain) in more detail than with the naked eye, provided that there are no image artefacts in these regions. Guidelines in adult cardio-oncology have adopted a reduced global longitudinal strain as an early sign of cardiotoxicity and specific strain patterns point to specific myocardial diseases (e.g. apical sparing in cardiac amyloidosis). It furthermore has high potential to aid in the indication for cardic resynchronization therapy by assessment of dyssynchronous patterns. However, the inclusion of myocardial strain analyses in systolic function quantification guidelines has been hampered by the lack of uniform lower limits of normal. These still depend on the software vendor, and furthermore on the myocardial layer in which strain is assessed and the timing of events. Attempts to resolve these problems are undertaken by a dedicated standardization task force.
Our research aim
For cardiac imaging, our current research aims to identify additional clinical applications of deformation imaging and deeper analysis of its current applications. The fields of research include pediatric cardio-oncology and congenital heart disease.
Methods
In the past, we have focussed on the development of strain estimation techniques in two-dimensional and three-dimensional echocardiography data. Currently, we provide an infrastructure with different software packages and technical support to clinicians and clinical studies that involve two-dimensional myocardial strain imaging. Cohort and case-control studies are hosted that compare the hearts of childhood cancer survivors to controls and that assess the hearts of patients with Ebstein anomaly in further detail. Furthermore, we undertake continuous efforts to provide lab- and vendor specific normative strain values.
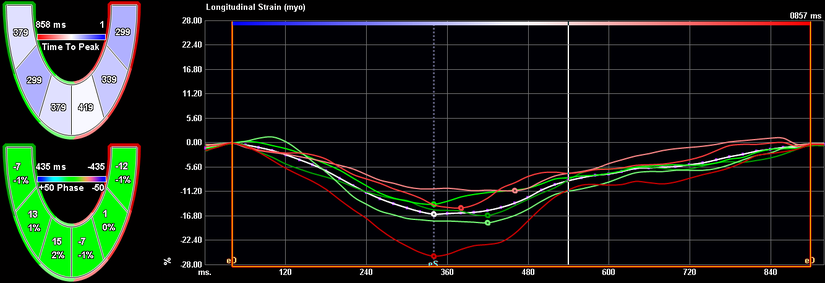
example of regional (coloured) and average (white) longitudinal strain curves in an apical 4-chamber view in a childhood cancer survivor, obtained in commercially available, vendor-independent strain software.
Results
We have developed 2D and 3D strain estimation and segmentation strategies to improve improve accuracy with respect to commercially available techniques. These strategies are based on analysis of the raw ultrasound (rf) signals: rf-based strain estimation demonstrated to be more accurate than B-mode based commercial techniques (Lopata et al 2009, Lopata et al 2009a, Lopata et al 2009b) and these techniques were extended from 2D to biplane strain imaging (Lopata et al 2010) and full 3D (Lopata et al 2011). Automated segementation based on echo statistics (Nillesen et al 2008)) and decorrelation (Nillesen et al 2009) were developed and validated in vivo (Nillesen et al 2009a) and finally evaluated in children with congenital heart disease (Nillesen et al 2011).
Furthermore, clinical application of strain and strain rate with tissue Doppler (Kapusta et al., 2000a, 2000, 2001,) and speckle tracking in childhood cancer survivors (Mavinkurve-Groothuis et al., 2010, 2012; Pourier et al., 2020; Merkx et al., 2021a, 2021b) ) has advanced this field of subclincial detection of cardiac dysfunction.
Most recently, we described our 15-year experience with measuring myocardial strain in the surveillance of childhood cancer survivors and its potential value over LVEF predicting 10-year cardiac events (Pourier et al., 2022).
Funding
- Detection of chronic heart failure in children with congenital heart disease with innovative ultrasound techniques (Dutch Technology Foundation STW and Philips Medical Systems, finished)
- Early recognition of cardiovascular disease (Dutch Heart Foundation CVON 2015-021, finished)